
青藏高原就医可达性格局演变及其影响因素
|
高兴川(1987—),男,博士,副教授,研究方向为智慧交通与区域发展。E-mail:gaoxch@foxmail.com |
收稿日期: 2024-08-29
修回日期: 2024-11-13
网络出版日期: 2025-08-07
基金资助
国家自然科学基金项目(42101207)
国家自然科学基金项目(42101170)
浙江省自然科学基金项目(LTGG24D010001)
科技部第二次青藏高原综合科学考察研究项目(2019QZKK0406)
Spatial Pattern Evolution and Influencing Factors of Accessibility to Medical Treatment in the Qinghai-Xizang Plateau
Received date: 2024-08-29
Revised date: 2024-11-13
Online published: 2025-08-07
高兴川 , 张雯婷 , 马仁锋 . 青藏高原就医可达性格局演变及其影响因素[J]. 经济地理, 2025 , 45(6) : 100 -108 . DOI: 10.15957/j.cnki.jjdl.2025.06.010
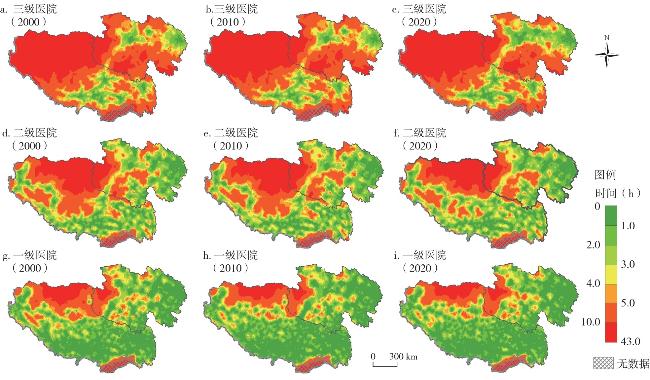
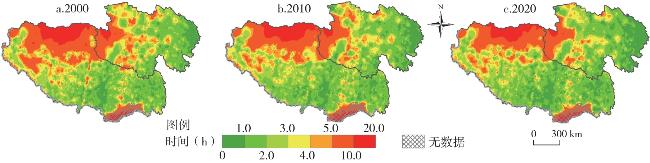
The accessibility and service capacity of medical facilities are crucial for ensuring the health of residents. Under the background of the impetus of the system of tiered diagnosis and treatment and Healthy China, this study analyzes the accessibility of medical service facilities at different levels in the Qinghai-Xizang Plateau in 2000, 2010, and 2020. It explores the spatial-temporal dynamics of integrated healthcare accessibility at the township scale, with consideration of service utilization probability, analyzes its spatial heterogeneity in correlation with population distribution, and identifies the determinants affecting these patterns. The results show that: 1) From 2000 to 2020, there has been a significant improvement in the accessibility to medical treatment in the Qinghai-Xizang Plateau, the short-term accessibility coverage area gradually expands and showing an inverse correlation with hospital tier levels. The coverage area and population proportion of the isochrone circles (≤1 h) for primary-, secondary-, and tertiary-level hospitals are gradually increasing. 2) Taking into account the comprehensive accessibility of medical facilities with the probability of medical treatment, the coverage area and population proportion of the isochrone circles (≤ 1 hour and > 10 hours) are smaller than that of the comprehensive accessibility considering only the time cost. 3) The supply and demand relationship of comprehensive medical accessibility at the township scale has significant regional differentiation characteristics. Among them, the number of townships with high-high agglomeration has decreased, mainly transforming into a low-high type. The number of low-high type and low-low type of townships shows an increasing trend. 4) The density of hospital locations is the main influencing factor for the comprehensive accessibility of medical facilities at the township level, follow by altitude, road network density. GDP and population density also have a certain impact.
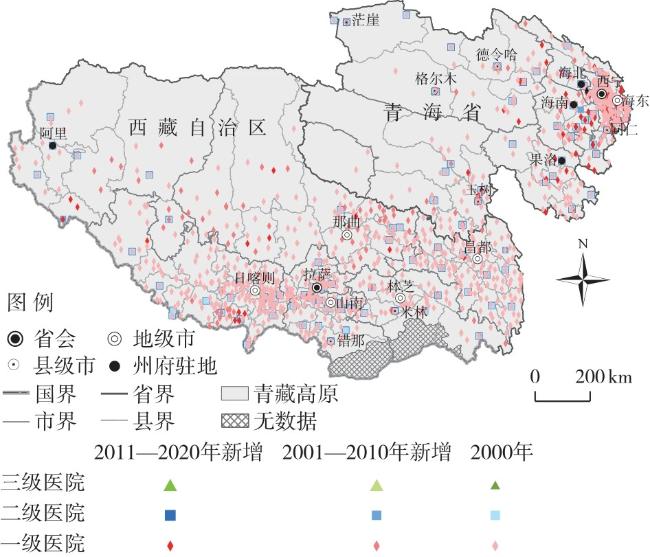
图1 研究区区位及医疗设施空间分布注:该图下载于自然资源部标准地图服务网站中审图号为GS(2020)4632的标准地图,底图无修改。 Fig.1 Location of research area and spatial distribution of medical facilities in the Qinghai-Xizang Plateau |
表1 青藏高原医疗资源数量情况Tab.1 Quantity of medical resources in the Qinghai-Xizang Plateau |
| 地区 | 医疗资源 | 2000 | 2010 | 2020 |
|---|---|---|---|---|
| 青海 | 每千人口医疗卫生机构床位数(张/千人) | 3.2 | 3.6 | 7.0 |
| 每千人口卫生技术人员数(人/千人) | 3.9 | 4.3 | 8.3 | |
| 综合医院(家) | 437 | 496 | 699 | |
| 西藏 | 每千人口医疗卫生机构床位数(张/千人) | 2.44 | 3.02 | 5.19 |
| 每千人口卫生技术人员数(人/千人) | 3.22 | 3.44 | 6.20 | |
| 综合医院(家) | 712 | 784 | 874 |
表2 青藏高原2000—2020年不同层级就医可达性等时圈覆盖面积比例(%)Tab.2 Proportion of coverage area of medical treatment accessibility for the different hospital tier levels in the Qinghai-Xizang Plateau from 2000 to 2020 (unit: %) |
| 等级 | 年份 | ≤1 h | 1~2 h | 2~3 h | 3~4 h | 4~5 h | 5~10 h | >10 h |
|---|---|---|---|---|---|---|---|---|
| 三级 医院 | 2000 | 1.75 | 4.60 | 6.59 | 7.54 | 8.86 | 31.42 | 39.24 |
| 2010 | 1.76 | 4.59 | 6.60 | 7.52 | 8.86 | 31.43 | 39.25 | |
| 2020 | 3.30 | 6.81 | 7.50 | 7.98 | 8.49 | 28.87 | 37.05 | |
| 二级 医院 | 2000 | 11.46 | 15.50 | 14.01 | 14.01 | 8.67 | 22.07 | 16.58 |
| 2010 | 11.91 | 15.58 | 14.31 | 11.72 | 8.48 | 21.69 | 16.57 | |
| 2020 | 13.83 | 16.99 | 15.76 | 12.01 | 7.71 | 18.54 | 15.18 | |
| 一级 医院 | 2000 | 38.66 | 19.26 | 11.16 | 7.97 | 5.11 | 11.18 | 6.68 |
| 2010 | 38.66 | 19.26 | 11.16 | 7.97 | 5.11 | 11.18 | 6.68 | |
| 2020 | 39.26 | 18.26 | 10.73 | 7.74 | 5.05 | 11.88 | 7.09 |
表3 青藏高原2000—2020年不同层级就医可达性等时圈覆盖人口比例(%)Tab.3 Population proportion of medical treatment accessibility for the different hospital tier levels in the Qinghai-Xizang Plateau from 2000 to 2020 (unit: %) |
| 等级 | 年份 | ≤1 h | 1~2 h | 2~3 h | 3~4 h | 4~5 h | 5~10 h | >10 h |
|---|---|---|---|---|---|---|---|---|
| 三级 医院 | 2000 | 16.45 | 18.42 | 13.35 | 10.26 | 8.71 | 18.74 | 14.06 |
| 2010 | 16.65 | 16.59 | 12.71 | 10.16 | 8.81 | 18.98 | 16.10 | |
| 2020 | 47.42 | 11.86 | 6.84 | 5.53 | 4.89 | 11.49 | 11.98 | |
| 二级 医院 | 2000 | 43.87 | 20.28 | 11.16 | 6.49 | 3.80 | 7.21 | 7.20 |
| 2010 | 46.23 | 17.81 | 9.93 | 5.34 | 3.69 | 7.65 | 9.35 | |
| 2020 | 66.64 | 10.79 | 5.63 | 3.10 | 1.67 | 3.77 | 8.39 | |
| 一级 医院 | 2000 | 70.40 | 11.81 | 4.14 | 1.93 | 1.67 | 3.57 | 6.48 |
| 2010 | 72.96 | 8.83 | 3.02 | 1.79 | 1.73 | 3.62 | 8.05 | |
| 2020 | 82.33 | 4.55 | 1.50 | 0.83 | 0.88 | 2.17 | 7.73 |
表4 不同情景下综合就医可达性等时圈覆盖面积比例(%)Tab.4 Proportion of coverage area of isochrone circles for comprehensive medical treatment accessibility under different scenarios (unit: %) |
| 不同情景 | 年份 | ≤1 h | 1~2 h | 2~3 h | 3~4 h | 4~5 h | 5~10 h | >10 h |
|---|---|---|---|---|---|---|---|---|
| 未考虑 就诊概率 | 2000 | 33.62 | 18.66 | 11.92 | 8.28 | 5.70 | 13.82 | 8.01 |
| 2010 | 38.93 | 19.21 | 11.00 | 7.96 | 5.07 | 11.16 | 6.68 | |
| 2020 | 40.95 | 19.06 | 10.50 | 7.29 | 4.62 | 10.93 | 6.67 | |
| 考虑就 诊概率 | 2000 | 6.34 | 25.74 | 19.42 | 14.13 | 9.81 | 18.10 | 6.48 |
| 2010 | 8.35 | 29.24 | 19.59 | 12.78 | 8.78 | 15.28 | 5.99 | |
| 2020 | 12.89 | 29.35 | 18.50 | 12.50 | 7.39 | 14.59 | 4.77 |
表5 不同情景下综合就医可达性等时圈覆盖人口比例(%)Tab.5 Population proportion of isochrone circles for comprehensive medical treatmetn accessibility under different scenarios (unit: %) |
| 不同情景 | 年份 | ≤1 h | 1~2 h | 2~3 h | 3~4 h | 4~5 h | 5~10 h | >10 h |
|---|---|---|---|---|---|---|---|---|
| 未考虑 就诊概率 | 2000 | 37.90 | 32.99 | 11.76 | 4.42 | 2.77 | 4.50 | 5.66 |
| 2010 | 45.18 | 30.56 | 8.23 | 2.79 | 2.16 | 4.41 | 6.67 | |
| 2020 | 82.40 | 4.60 | 1.40 | 0.80 | 0.90 | 2.10 | 7.80 | |
| 考虑 就诊概率 | 2000 | 32.69 | 35.05 | 13.81 | 5.26 | 3.47 | 4.79 | 4.93 |
| 2010 | 40.29 | 32.19 | 9.16 | 3.57 | 2.58 | 5.89 | 6.32 | |
| 2020 | 63.20 | 19.40 | 4.50 | 1.90 | 0.90 | 4.00 | 6.10 |
表6 空间自相关不同集聚类型的乡镇数量Tab.6 Number of townships with different types of spatial autocorrelation |
| 年份 | 低—低型(个) | 低—高型(个) | 高—低型(个) | 高—高型(个) |
|---|---|---|---|---|
| 2000 | 168 | 109 | 10 | 153 |
| 2010 | 158 | 132 | 18 | 140 |
| 2020 | 193 | 196 | 10 | 111 |
表7 青藏高原乡镇尺度综合就医可达性影响因素相对作用强度(p<0.05)Tab.7 Relative strength of factors influencing comprehensive medical treatment accessibility in the Qinghai-Xizang Plateau at the township level |
| 年份 | 海拔 | 医院点密度 | 路网密度 | GDP | 人口密度 | 城镇化率 |
|---|---|---|---|---|---|---|
| 2000 | 0.1478 | 0.5026 | 0.2139 | 0.0696 | 0.0661 | - |
| 2010 | 0.1607 | 0.4947 | 0.1386 | 0.1155 | 0.0905 | - |
| 2020 | 0.1717 | 0.5130 | 0.1391 | 0.1087 | 0.0674 | - |
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
刘若杨, 史培军, 唐海萍, 等. 青藏高原植被产氧量及其对近地表大气氧含量的贡献率[J]. 地理学报, 2023, 78(5):1136-1152.
|
| [5] |
张俊, 姜海宁, 张文忠, 等. 2009—2018年西藏人口与经济的非均衡格局及其影响因素[J]. 地理研究, 2023, 42(1):172-190.
|
| [6] |
|
| [7] |
刘寿, 张发斌, 黄明玉, 等. 青海省卫生人力资源对分级诊疗实施影响分析[J]. 中国公共卫生, 2016, 32(4):531-534.
|
| [8] |
李继霞, 刘涛, 霍静娟. 中国农村公共服务供给质量时空格局及影响因素[J]. 经济地理, 2022, 42(6):132-143.
|
| [9] |
毛阳海. 推进西藏高原经济高质量发展的内在逻辑和实践路径[J]. 西藏民族大学学报(哲学社会科学版), 2023, 44(6):79-86.
|
| [10] |
陈文烈, 张秋雯. 青海经济高质量增长的“多元动力”——基于生态文明的基本内核与逻辑框架[J]. 青海民族大学学报(社会科学版), 2020, 46(3):39-47.
|
| [11] |
|
| [12] |
|
| [13] |
苗毅, 戴特奇, 王成新, 等. 青藏高原县域交通优势度—自然环境承载—社会经济需求关系评估[J]. 中国人口·资源与环境, 2023, 33(10):165-174.
|
| [14] |
|
| [15] |
刘庆芳, 宋金平. 青藏高原县域人口与公共服务适配性与优化策略[J]. 经济地理, 2022, 42(10):43-51.
|
| [16] |
|
| [17] |
荣旖旎, 欧阳文静. 公路可达性对农村居民县城就医行为的影响——来自村庄月度数据[J]. 经济地理, 2024, 44(3):45-54.
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
吴晓凡, 干颖滢, 尹悦, 等. 拉萨市医疗卫生服务现状及空间可达性研究[J]. 中国卫生经济, 2023, 42(3):25-29.
|
| [23] |
刘泽, 程杨, 陶卓霖, 等. 西藏自治区层级医疗设施可达性精细化评价[J]. 地理学报, 2024, 79(2):502-514.
|
| [24] |
孔劲松, 程杨, 陶卓霖. 青藏高原居民医疗服务满意度及影响因素研究[J]. 中国卫生事业管理, 2023, 40(7):520-525.
|
| [25] |
中共中央国务院. “健康中国2030”规划纲要[EB/OL]. 中国政府网, https://www.gov.cn/zhengce/2016-10/25/content_5124174.htm, 2016-10-26.
|
| [26] |
张镱锂, 李炳元, 刘林山, 等. 再论青藏高原范围[J]. 地理研究, 2021, 40(6):1543-1553.
|
| [27] |
洁安娜姆. 健康中国战略的理论蕴涵及其在西藏的实践[J]. 西藏发展论坛, 2023(2):78-83.
|
| [28] |
陈芃, 刘永年, 黄明玉, 等. 需方对分级诊疗制度的满意度分析——以青海省为例[J]. 青海医学院学报, 2015, 36(4):280-283.
|
| [29] |
|
| [30] |
高兴川, 曹小曙, 李涛, 等. 1976—2016年青藏高原地区通达性空间格局演变[J]. 地理学报, 2019, 74(6):1190-1204.
|
| [31] |
|
| [32] |
胡舒云, 陆玉麒, 胡国建, 等. 基于多源大数据的深圳市医疗设施可达性与公平性测算[J]. 经济地理, 2021, 41(11):87-96.
|
| [33] |
|
| [34] |
|
| [35] |
国家卫生计生委统计信息中心. 2013第五次国家卫生服务调查分析报告[R]. 国家卫生健康委员会, 2016.
|
| [36] |
王劲峰, 徐成东. 地理探测器:原理与展望[J]. 地理学报, 2017, 72(1):116-134.
|
| [37] |
杨珍, 王伟, 陈准, 等. 分级诊疗制度下洛阳市医疗服务空间可达性及影响因素研究[J]. 河南大学学报(自然科学版), 2024, 54(2):142-156.
|
| [38] |
刘昊鹏, 马骋宇, 杨彦彬, 等. 北京市山区与平原郊区村级医疗服务可达性评价——基于调查的2SFCA研究[J]. 中国卫生政策研究, 2024, 17(7):65-74.
|
| [39] |
刘泽, 张娜娜, 程杨, 等. 青海省医疗资源配置的空间公平与效率评价[J]. 地理科学进展, 2023, 42(10):1891-1903.
|
| [40] |
|
/
| 〈 |
|
〉 |


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}